- Research
- Open access
- Published:
Egyptian evidence-based consensus on clinical practice recommendations for the management of systemic sclerosis
Egyptian Rheumatology and Rehabilitation volume 51, Article number: 9 (2024)
Abstract
Background
This work aims to develop clinical practice recommendations for the management of systemic sclerosis (SSc).
Results
Fourteen expert panels had completed the two rounds of surveys. After the end of round 2, recommendations were released and distributed on 11 domains. The percentage of the agreement on the recommendations was 92.3% to 100%. All 11 key questions were answered at the end of the second round with agreement.
Conclusion
This guideline tried to tackle the gaps in research that limit treatment options. Stratifying the patients according to their disease domains has helped to set up sequential management pathways for each domain.
Background
Systemic sclerosis (SSc) is a rare autoimmune rheumatic disease [1] characterized by skin fibrosis, vasculopathy as well as internal organs affection. Due to its diverse, complex, and multi-systemic nature, the lack of a specific diagnostic test, and how the disease might initially present itself, there is a delay in the diagnosis process associated with a high degree of uncertainty regarding what complications may arise and how to manage it [2]. Consequently, this represents a challenge for both the patients and the physicians. In comparison to all the other autoimmune rheumatic diseases, SSc has the highest mortality, with approximately 70% of the affected patients eventually dying due to the illness itself or a result of its systemic complication [3].
In a trial to tackle the mosaic nature of the disease and following the consideration of early SSc definition [4], the American College of Rheumatology (ACR) and The European Alliance of Associations for Rheumatology (EULAR) jointly proposed guidelines for Systemic Sclerosis classification [5]. Such criteria facilitate the earlier diagnosis of the disease, at stages when the illness might potentially be amenable to therapy. In fact, such advances in understanding the disease’s pathognomonic features, evolving criteria for early diagnosis and newer therapeutic modalities provide a new ray of hope in this disease.
With imperative new drug trials and evidence-based therapies for the management of SSc, together with changes in medical care policies in Egypt and the introduction of the national insurance strategy; it was important to provide a practical roadmap for the treatment of SSc. Therefore, the aim of this work is to develop a guideline that builds upon the previously published management guidelines and incorporates recent developments in evidence-based medical therapies as well as increased knowledge about the evaluation, classification, and investigations of systemic sclerosis.
Methods
Design
The study design was developed through a qualitative synthesis of consensus and scientific evidence, using both clinical experience and currently available scientific evidence. The “Clinical, Evidence-based, Guidelines” (CEG) initiative procedure was followed in this multi-step process, which sought to establish an actionable clinical gold standard for Treat-to-Target management of rheumatic and bone diseases. The manuscript's evidence-based section complied with the recommended reporting items for systematic reviews and the meta-analyses reporting requirements for systematic reviews [6]. The Egyptian Academy of Rheumatology spearheaded the effort.
Development stages
Core team
It is formed of three experts with established experience in rheumatology, particularly SSc. The core team coordinated and supervised the teamwork, and assisted in the development of the project scope and setting up of the initial Patient/Population, Intervention, Comparison, and Outcomes (PICO) [7] clinical questions. The team has also helped in reaching a consensus on the key questions to be included in the guideline nominating the expert panel and drafting the manuscript.
Literature review team
Led by 1 methodologist and 2 experienced specialists in review of the literature with the base of key research questions, were identified. The task was to carry out review of the literature [8] focussing on SSc diagnosis and treatment. The period covered by the article search was January 2000–July 2023.
Data sources and search strategies
The Key clinical questions (Table 1) were used to conduct the literature search. The bibliographic research was carried out until July 2023, to find studies that met the criteria for inclusion in the MEDLINE, EMBASE, and Cochrane Library databases. For pragmatic reasons, the language was limited to English. The search strategies were designed to be broad to have high sensitivity for identifying relevant literature.
This systematic review was conducted following the specific Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) methodological guidelines [6] and the PICO question model for the definition of the inclusion criteria: P (population): “systemic sclerosis patients”; I (intervention): “treatment”, “treatment with biologic medications”; C (comparison): “same conditions with placebo, sham therapy or no intervention or pre-/post-comparison data group”; O (outcomes): “Skin disease (modified Rodnan scale value [mRSS]); pulmonary function test (forced vital capacity [FVC] and carbon monoxide diffusing capacity [DLCO]); and health status (Health Assessment Questionnaire [HAQ] Disability Index [DI] → HAQ-DI Scale). These parameters were included as outcomes as they are commonly assessed in health biomarker studies and in SSc research [9].
Bibliographic search terms included a mix of medical subject headings (MeSH) and free text words for key concepts related to SSc: scleroderma, systemic sclerosis, scleroderma diffuse, diffuse cutaneous systemic sclerosis, guidelines, consensus, recommendation, best practice, therapeutics, biologic therapy, rituximab, nintedanib, ofev, tocilizumab, azathioprine, biological therapy, DMARDs, antibodies, and monoclonal (monoclonal antibodies); all linked using the Boolean operators OR and AND.
Electronically, duplicate screening of the findings of the literature search was done. By looking through the reference lists of studies found using the database search methodologies that satisfied the inclusion requirements, further pertinent research was found. Following the revision, each of the experts responsible for the literature review provided recommendations regarding each section based on evidence, when that was available, or on their own experience.
Level of evidence
Levels of evidence are assigned to studies based on the research design, quality of the study, and applicability to patient care. The level of evidence was determined for each section using the Oxford Centre for Evidence-based Medicine (OCEBM) system (Supplement Table S2) [10]. Higher levels of evidence have less risk of bias.
Study selection
By using inclusion and exclusion criteria for the literature that was found using the search methodologies, the pertinent studies were chosen.
Inclusion criteria
The included articles were observational studies, case–control, cohort, and cross-sectional studies; systematic reviews; uncontrolled trials; and randomized controlled trials (RCTs). When multiple publications reported data from the same study, the publication with the most complete data was included whereas publications reporting duplicate data were excluded. Studies were reviewed for inclusion or exclusion in two stages—first, titles and abstracts were assessed, and then studies identified as possibly relevant by title/abstract screen received full-text review.
Exclusion criteria
Editorials, conference abstracts, commentary, and narrative/personal reviews that lack supporting data were not included.
Study selection and data extraction
All reports were independently screened for inclusion by two reviewers. A third expert was consulted in the event that there was a dispute. Every report’s year of publication, study design, number of patients, kind, severity, and duration of the SSc, dosage and/or dosing schedule, duration of treatment, definition of effective treatment, outcome, side effects, and the number of dropouts and their causes were noted.
Expert panel
Fourteen members were nominated by the core leadership team. Their selection criteria included being actively involved in scientific research on SSc and having at least 10 years of experience in their specialty (rheumatology, dermatology, cardiovascular, pulmonology, gastroenterology, or nephrology). Information on the project’s objective and the Delphi approach were included in the invitation that was sent to the experts. The experts who accepted this invitation were informed that in order to take part in the next rounds of ratings, they had to reply to the first round. The expert panel participated in the project’s scope development, helped to improve the PICO questions, and submitted votes on the recommendations.
Key questions used to develop the guideline
The target population, classification criteria, intervention or exposure under investigation, comparison(s) used, outcomes used to measure efficacy, effectiveness, or risk, and the timing of introducing the appropriate management are all defined by a set of structured key questions that served as the basis for this guideline. The following procedures were followed in order to collect the evidence needed to respond to the clinical questions: developing the clinical questions, organizing the questions, searching for evidence, critically evaluating and choosing the evidence, presenting the findings, and making recommendations. These inquiries, as indicated in Table 1, serve as the basis for the systematic literature search and, subsequently, the clinical care standards.
Developing the clinical care standards framework
Based on the answers to the structured key questions and the literature research, a structured template was developed to assist in the standardized identification of the recommendation components. It has been determined what format each component’s information and recommendations would be retrieved and presented in.
Delphi process
Thus, the Delphi method’s aim is to generate consensus recommendations from a panel of experts through an organized, iterative process. The two main characteristics of this approach are participant anonymity and regulated feedback [11,12,13].
Consensus process
From 4 to 27 October 2023, to reach a consensus, there were two Delphi rounds. Following the identification of the main aspects of this strategy, a working group with the scientific committee determined which components should be included in the surveys. The structured Delphi method, which is particularly useful for geographically disparate centers like Egypt, guarantees that participant perspectives are taken into equal consideration. Online questionnaires were used to carry out the Delphi process. Two rounds were used as this is seen to be the best way to achieve consensus and allows for sufficient reflection on group responses [14]. Additionally, free-text answers from round 1 could be added to round 2 surveys in two rounds as new statements. There were 11 domains in the initial electronic questionnaire round.
Voting process
Voting was conducted in two time-limited rounds via live online distribution. Every task force member received an invitation to participate and advance notice of the start and end times of each voting session. Votes were collected and processed anonymously, and special access links were distributed. During the voting process, feedback on possible ambiguity, unidentified overlaps, and rephrasing of each statement was received. Voting on the statements was restricted to task force members alone.
Rating
Every statement received a score ranging from 1 to 9, where 1 represented “complete disagreement” and 9 represented "complete agreement." In general, the numbers 1–3, 4–6, and 7–9 stand for disagreement, uncertainty, and agreement, in that sequence. If a member feels that a statement is outside of their area of competence, they are advised to abstain. Consequently, “inconvenience about the accuracy of the recommendation” is represented by a “uncertainty” vote. Following each voting round, comments that were examined by the scientific committee are permitted for all statements. Members were also encouraged to offer comments in each voting round when they disagreed with a decision. This will enable the panel to identify cases of misinterpretation of statements and nullify the vote on those specific statements.
Definition of consensus
An agreement-based definition was created before any data was analyzed. It was discovered that consensus would be formed if at least 75% of participants achieved agreement (score 7–9) or disagreement (score 1–3) [8, 11, 12]. A statement was retired if its mean vote fell below three or it had a “low” degree of agreement. Statements that scored between 4 and 6 on the uncertainty scale had their rates changed in light of the feedback. Each recommendation statement's levels of agreement were classified as “high” if, following the second round of voting, every vote fell inside the agreement bracket (7–9) [13, 15, 16]. When replies varied by less than 10% between round groups, stability of consensus was deemed to have been attained [17].
Chronogram of Delphi rounds
The first round ran for 9 days, from October 4–12, 2023. In consideration of the feedback, the elements on which respondents were unable to reach consensus in the first round were changed and included in the second. The second round was held from October 20–27, 2023, for 8 days, 1 week after the first round.
Ethical aspects
The Helsinki Declaration was followed in the conduct of this study. This involved a series of steps that adhered to the “Clinical, Evidence-based, Guidelines” (CEG) initiative protocol (Tanta University’s ethical board, ethical approval code: 34,842/8/21). The process’ objective was to establish a practical clinical gold standard for Treat-to-Target management of bone and rheumatic diseases.
Results
Literature research and evidence selection
Nine hundred forty-five records were found during the search; 714 of those were reviewed after duplicates were eliminated (231). We were able to obtain the complete text of 115 possible papers after screening. The literature review contained 24 papers. The findings were compiled, summarised, and developed into suggestions for the care of SSc patients. After that, they were debated, changed, and put to a vote. Supplementary Figure S1 displays this process’s flowchart.
Expert panel characteristics
The Delphi form was sent to the expert panel (n = 14) all the panels completed the two-round survey. The participants were one from Europe and 13 from Africa (Egypt).
Delphi round 1
Eleven topics, all of which addressed clinical questions addressed in later rounds, made up the round devoted to the major clinical questions. Every domain and question was accepted (all respondents strongly agreed or agreed), and no questions were removed from the list.
Delphi round 2
Using the data from round 1, a list of 11 sectioned recommendations was produced based on the literature search. The experts' panel received 100% of the responses for round 2. Changes in wording were proposed for eight domain statements. The claims were updated and changed. There was agreement on every point (more than 80% of respondents strongly agreed or agreed). The ratings given by medical professionals and patients did not differ much. The gastrointestinal and vascular domains were the focus of the primary modification.
Statements and grade of recommendations (GOR) for the management of SSc
The following is a list of the recommendations made in order to address the main clinical questions. Under each section are the following: the mean degree of agreement among the expert panel members, the percentage of agreement, the level of evidence (LOE), and the grades of recommendations. Table 2 shows the overarching principles for these recommendations.

Chronological affection of skin and organ affection in diffuse cutaneous systemic sclerosis

Chronological affection of skin and organ affection in limited cutaneous systemic sclerosis
There are 11 domains to answer the 11 key questions.
-
1
What is the aim of this guideline? level of agreement: Mean + SD: 8.92 ± 0.28, percentage of agreement: 100%, Level of agreement: High.
The purpose of the guideline is to support medical professionals who treat and care for individuals with systemic sclerosis in all of its clinical manifestations. Patients and those in charge of procuring systemic sclerosis patient care in the National Health Service should find the guideline to be a useful resource.
-
2.
Who are the targeted audience? level of agreement: Mean + SD: 8.85 ± 0.55, percentage of agreement: 100%, Level of agreement: High
Management of SSc should occur within the framework of a multidisciplinary team. Therefore, this recommendation is for rheumatologists, dermatologists, pulmonologists, cardiologists, and other physicians who are involved in the management of SSc patients.
-
3.
What is the classification of Systemic Sclerosis/localized scleroderma? level of agreement: Mean + SD: 8.61 ± 0.5, percentage of agreement: 100%, Level of agreement: High
When SSC is suspected clinically by the expert physician; ANA and capillaroscopy should be done for early diagnoses and management, then cardiopulmonary consultation could be done. SSc are classified according to Systemic Sclerosis 2013 ACR/EULAR classification criteria. Clinical presentation can be either localized scleroderma or systemic sclerosis according to the clinical presentation and the visceral involvement. Localized scleroderma is limited to fibrotic involvement of the skin and subcutaneous tissues (morphea or linear scleroderma), while SSc affects also internal organs which is classified as limited cutaneous or diffuse cutaneous type (Diffuse proximal skin involvement is defined as involving the skin of the trunk or proximal limbs). Rarely SSc could be presented as SSc sine scleroderma in the absence of cutaneous sclerosis.
It is important to identify those with overlap disease so that SSc can be administered concurrently with the overlap features.
-
4.
What are the benefits of classification or stratification of systemic sclerosis? level of agreement: Mean + SD: 8.85 ± 0.53, percentage of agreement: 100%, Level of agreement: High
It's important to distinguish between localized scleroderma and systemic sclerosis, as they differ in their management approaches. SSc should also differentiated into limited cutaneous and diffuse cutaneous types; as they are different in their specific autoantibodies, associated with different presentations in internal organ manifestations, and differ in prognosis and outcomes. Also, classification helps to differentiate SSc from scleroderma mimics.
-
5.
How to evaluate and follow-up systemic sclerosis patient? Level of evidence: 4C, level of agreement: Mean+SD: 8.85 ± 0.38, percentage of agreement: 100%, Level of agreement: High
-
Baseline organ-specific evaluation and monitoring should be done when any organ or system affection is suspected.
-
Follow-up examinations are essential for screening and monitoring the complications and visceral damage, disease activity and severity, and monitoring the treatment effect, tolerability, and adverse effects.
-
Monitoring of SSc patients differs according to organ affection, type of complication, and severity of disease. Unless there is an emergency or life-threatening condition, follow-up should be done every 3 months, especially in the first 5 years of onset of the disease then every 6 months.
-
-
6.
How to screen for organ involvement in SSc? Level of evidence: 3C, level of agreement: Mean + SD: 8.85 ± 0.38, percentage of agreement: 100%, Level of agreement: High
-
For early evaluation of SSc; capillaroscopy should be done which has diagnostic, prognostic, and disease activity assessment roles.
-
Laboratory assessment is crucial in classification and prognostic values of SSc (Fig. 3), such that:
-
Anti-Scl-70 (anti-topoisomerase) antibody is associated with dcSSc, and a higher risk for the development of progressive interstitial lung disease (ILD),
-
Anticentromere antibody (ACA) is associated with lcSSc, the risk for pulmonary artery hypertension (PAH), and primary biliary cirrhosis.
-
Positive RNA polymerase III antibody is at the highest risk of developing scleroderma renal crisis (SRC), and heart affection.
-
Anti-fibrillin is associated with PAH and cardiac affection, and anti-U1RNP is associated with overlap, mixed connective tissue disease (MCTDs), and lung fibrosis. Anti-PM-Scl is associated with myositis
Fig. 3 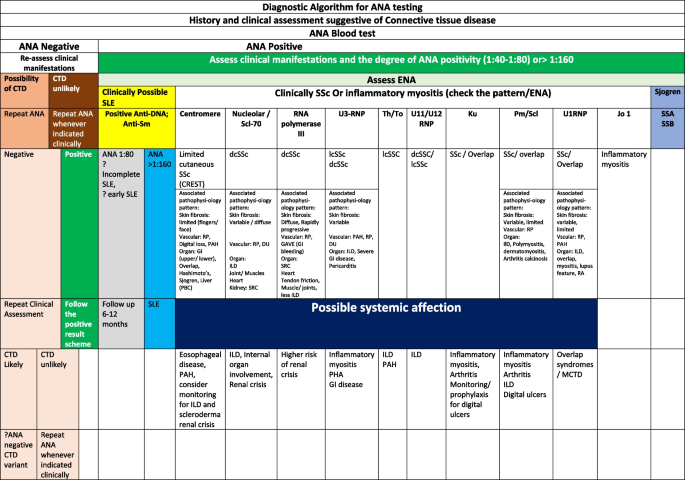
Diagnostic algorithm for ANA testing
-
-
Cardiopulmonary evaluation [pulmonary function tests (PFTs), high-resolution CT (HRCT) chest, ECHO cardiography, or even cardiac catheterization] should be done as early as possible when suspected cardiopulmonary affection in SSC patients.
-

-
7.
What are the general recommendations in the management of early SSc? Level of evidence: 3C, level of agreement: Mean + SD: 8.69 ± 0.48, percentage of agreement: 100%, Level of agreement: High.
-
Early recognition and diagnosis of dcSSc is a priority, with referral to a specialist SSc center
-
Early and accurate diagnosis = earlier intervention = more effective therapies
-
Evaluate every patient for organ involvement
-
Recognize associated factors and stratify risk
-
Screen early: Do not wait for symptoms to develop
-
Accurate physical examination can be very helpful
-
Assess for comorbidities
-
D-Penicillamine is not recommended.
-
Autologous hemopoietic stem cell transplant ASCT may be considered in some cases, particularly where there is a risk of severe organ involvement, balancing concerns about treatment toxicity.
-
-
8.
How to manage organ-specific affection of systemic sclerosis?
General principles for evaluation of organ involvement in SSc
-
Evaluate every patient for organ involvement
-
Recognize associated factors and stratify risk
-
Screen early—do not await for symptoms development
-
Accurate physical examination can be very helpful
-
Assess for comorbidities
Management of each system or organ in SSc is mentioned in detail in Table 3. The approach to Raynaud’s phenomenon and Digital Ulcer management is summarized in Table 4.
-
9.
What is the non-pharmacological management of systemic sclerosis? Level of evidence: 4D, level of agreement: Mean + SD: 8.69 ± 0.48, percentage of agreement: 100%, Level of agreement: High
-
Non-pharmacological therapies are recommended in all cases of SSC to avoid disability.
-
SSC patients must stop smoking and should do regular exercise as tolerated
-
Avoidance of cold exposure and protection against microtrauma is important for the management of Raynaud’s phenomena (RP-SSC).
-
Salt-reduced diet should be followed in patients with PAH and peripheral edema
-
Physiotherapy and rehabilitation modalities for the musculoskeletal system, pulmonary and cardiac rehabilitation
-
Occupational therapy is important, especially in patients with extensive hand affection.
-
Consultation with a dietitian and food modification are essential, especially in GIT affection.
-
Psychotherapy and social support are essential for SSC patients.
-
-
10.
What is the risk of malignancies in systemic sclerosis patient? (LOE 1 b) Level of evidence: 2B, level of agreement: Mean + SD: 8.61 ± 0.65, percentage of agreement: 100%, Level of agreement: High
-
All patients with new onset SSC should have a comprehensive physical examination and age-, sex- and risk factor-based cancer screening tests.
-
Scleroderma patients with positive RNA polymerase III and anti-topoisomerase I antibodies are at higher risk for malignancy.
-
Long-standing lung fibrosis is considered a lung cancer risk factors
-
Some patients with SSc and chronic GERD develop Barrette’s esophagus, which can progress to dysplasia, which is a risk factor for esophageal adenocarcinoma.
-
Exposure to cyclophosphamide is linked to bladder cancer.
-
-
11.
What are the serious complications and prognosis of systemic sclerosis? Level of evidence: 4C, level of agreement: Mean + SD: 8.85 ± 0.37, percentage of agreement: 100%, Level of agreement: High
-
The prognosis of SSC differs widely according to depending on the type of cutaneous affection and the type and degree of visceral affection.
-
Diffuse cutaneous type is the worst prognosis and rapidly progressive type of SSc especially in the first 3–5 years from disease onset. The most common associated complications are musculo-cutaneous complications, diffuse infiltrative lung disease, and/or cardiac symptoms, renal crisis, and gastrointestinal disorders (Fig. 1).
-
The most common complications associated with limited cutaneous SSc are PAH and digestive affection, other visceral affections are less common than diffuse type (Fig. 2).
-
The mortality rate is higher in the diffuse than limited cutaneous form of the disease.
-
Life-threatening conditions in SSc depend on the extent of major complications such as gastric antral vascular ectasia, intestinal pseudo-obstruction, SRC, ILD, PAH, and myocardial dysfunction.
-
Discussion
Systemic sclerosis represents, likely, a group of closely related systemic pathologies that share features of autoimmunity, vasculopathy, and fibrosis. Over the past decades, there has been an unmet need for clinical practice guidelines in the management of several domains in affected SSc patients. Consequently, it was paramount to provide a comprehensive management approach to SSc. The aim of this work was to develop a holistic standard clinical guideline valid to ensure the delivery of high-quality and homogeneous care for the management of SSc patients.
The developed guidelines provided global management of SSc, and in the meantime endorsed the patients’ stratification according to their risk. The guideline was grouped into 11 domains regarding assessment and management. This includes eight disease domains: Raynaud’s phenomenon and digital ulcers, skin, musculoskeletal, cardio-pulmonary, interstitial lung disease, gastrointestinal, renal, and neurological affection. Consequently, it suggested sequential treatment of SSc organ-based complications. The developed guideline endorsed also the awareness of the treating healthcare professionals regarding the high-risk probability of their patients developing organ-specific damage such as renal crisis or interstitial lung disease. Appropriate screening and treatment practices should be implemented to ensure long-term benefits. This is in line with recently published guidelines including the published EULAR recommendations [9, 18], the British Society for Rheumatology (BSR) guideline (2016) [19], the European Dermatology Forum Guideline [20], UK Scleroderma Study Group (UKSSG) best practice recommendations [21,22,23,24] and the single hub and access point for pediatric rheumatology in Europe recommendations on juvenile SSc [25].
The guidelines considered the role played by the disease pathophysiologic features in setting up the management pathway. An example is the recommendation of a similar medical therapy protocol for Raynaud’s, digital ulcers as well as pulmonary arterial hypertension, three well-known vascular manifestations of SSc, which in turn reflect the unified vascular phenotype in systemic sclerosis. This also raises the attention to the potential prophylactic impact of starting early treatment for one disease phenomenon which might benefit another belated one. This is important time-wise as pulmonary hypertension usually develops several years (around 10 years) after the first symptom (Fig. 1), so by treating Raynaud’s phenomena and digital ulcers, pulmonary hypertension may be prevented. This is supported by the available longitudinal studies, though they are few. Yet the more robust data from the EUSTAR [26] cohort suggest worse outcomes when a history of digital ulcers is present. Such therapeutic strategies pave the way to ‘widen’ the still very narrow ‘window of opportunity’.
The developed guideline endorsed also the use of targeted synthetic and biological therapies as disease-modifying medications for SSc key fibrotic manifestations. Mycophenolate mofetil has been recommended for the treatment of skin fibrosis. For SSc-associated interstitial lung disease, mycophenolate mofetil, Rituximab, tocilizumab as well as nintedanib have been suggested. On another front, phosphodiesterase-5 (PDE-5) inhibitors and endothelin receptor antagonist [ERA] monotherapy have also been recommended for up-front combination use for digital ulcers and pulmonary hypertension. Though these were present in 2017, recent clinical trials have discussed and confirmed the benefit of nintedanib, rituximab, or tocilizumab in SSc-associated interstitial lung disease [27, 28].
This guideline was developed with the best evidence and consensus across a range of expert opinions. Current management is essentially centered on the specialty of rheumatology with appropriate engagement and cross-referral to other specialties including respiratory medicine, dermatology, nephrology, gastroenterology, cardiology, and others. There are also important shared care links with other specialists. The expert panel that was shared in this work covered all these specialties including 9 rheumatologists, 1 methodologist, 1 respiratory medicine, 1 dermatologist, 1 cardiologist, 1 nephrologist, and 1 gastroenterologist. This was necessary to establish auditable criteria and guarantee that the care is coordinated. This agrees with the approach adopted in a series of best practice recommendations published earlier [18,19,20,21,22,23,24,25].
Such methodology has helped to harmonize management across expert healthcare professionals. The multidisciplinary strategy endorsed in this guideline is expected also to tackle another challenge that faces healthcare professionals managing SSc patients. This includes SSc patients presenting with a major organ-based complication such as renal crisis, interstitial lung disease, pulmonary artery hypertension, or thrombotic microangiopathy who have not yet been diagnosed with SSc although they may fulfill the 2013 ACR/EULAR classification criteria [5].
Limitations of the guideline
The guideline’s lack of comparative evidence to assist therapy selection and its low number of longitudinal studies, albeit reflecting the best available data at the time the report was created, are two of its weaknesses. The main comparative benefit/efficacy and harms evidence is incorporated here. The fact that we limited our search to works written in English is another drawback. When evaluating the data, care should be taken because the findings of more research may need to change the report's conclusions or suggestions. In the best interests of particular patients and unique situations, it can be required—even desirable—to deviate from the recommendations. Deviation from guidelines should not always be considered negligent, just as following them may not be sufficient to defend against a claim of carelessness.
Conclusion
There is a vascular as well as fibrotic disease continuum in systemic sclerosis. This guideline tried to tackle the gaps in research that limit treatment options. Stratifying the patients according to their disease domains has helped to set up sequential management pathways for each domain. This has also facilitated the recognition of common pathogenic pathways, which paved the way for identifying similar management patterns for different organ manifestations. Putting this recommendation into routine practice will hopefully result in better care for SSc patients as long as data support best practices in management. The consensus panel’s wide representation would help to spread the findings of this research to the many medical professionals who care for persons with schizophrenia, increasing the likelihood that the guidelines will be adopted and followed.
Availability of data and materials
The data will be available upon reasonable request.
Abbreviations
- ACR:
-
American College of Rheumatology
- ACA:
-
Anticentromere antibody
- BSR:
-
British Society for Rheumatology
- ds.SSC:
-
Diffuse cutaneous systemic sclerosis
- HRCT:
-
High-resolution CT
- ILD:
-
Interstitial lung disease
- lc.SSC:
-
Limited cutaneous systemic sclerosis
- MCTDs:
-
Mixed connective tissue disease
- CEBM:
-
Oxford Centre for Evidence-based Medicine
- PAH:
-
Pulmonary artery hypertension
- PFTs:
-
Pulmonary function tests
- RCTs:
-
Randomized controlled trials
- RP:
-
Raynaud's phenomena
- SRC:
-
Scleroderma renal crisis
- SSc:
-
Systemic Sclerosis
- CEG:
-
The Clinical, Evidence-based, Guidelines
- EULAR:
-
The European Alliance of Associations for Rheumatology
- LOE:
-
The level of evidence
- UKSSG:
-
UK Scleroderma Study Group
References
Royle JG, Lanyon PC, Grainge MJ, Abhishek A, Pearce FA (2018) The incidence, prevalence, and survival of systemic sclerosis in the UK Clinical Practice Research Datalink. Clin Rheumatol 37:2103–2111
Smith V, Scirè CA, Talarico R, et al (2019) Systemic sclerosis: state of the art on clinical practice guidelinesRMD Open 4:e000782. https://doi.org/10.1136/rmdopen-2018-000782
Misra DP, Chowdhury AC, Phatak S, Agarwal V (2015) Scleroderma: Not an orphan disease any more. World J Rheumatol 5(3):131–141. https://doi.org/10.5499/wjr.v5.i3.131
Avouac J, Fransen J, Walker UA, Riccieri V, Smith V, Muller C, Miniati I, Tarner IH, Randone SB, Cutolo M (2011) Preliminary criteria for the very early diagnosis of systemic sclerosis: results of a Delphi Consensus Study from EULAR Scleroderma Trials and Research Group. Ann Rheum Dis 70:476–481
van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, Matucci-Cerinic M, Naden RP, Medsger TA, Carreira PE (2013) 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum 65:2737–2747
Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE et al (2021) PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 372:160
Schardt C, Adams MB, Owens T, Keitz S, Fontelo P (2007) Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak 2007(7):16
Leclercq E, Leeflang MM, van Dalen EC, Kremer LC (2013) Validation of search filters for identifying pediatric studies. J Pediatr 162:629–634
Kowal-Bielecka O, Landewé R, Avouac J, Chwiesko S, Miniati I, Czirják L, Clements P, Denton C, Farge D, Fligelstone K et al (2009) EULAR recommendations for the treatment of systemic sclerosis: a report from the EULAR Scleroderma Trials and Research group (EUSTAR). Ann Rheum Dis 68:620–628
OCEBM Levels of Evidence Working Group (2011) The Oxford levels of evidence 2. Oxford Centre for Evidence-Based Medicine, Oxford, UK
Hsu CC, Sandford BA (2007) The Delphi technique: making sense of consensus. Practical assess Res Eval 12:1–8
Diamond IR, Grant RC, Feldman BM, Pencharz PB, Ling SC, Moore AM, Wales PW (2014) Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol 67(4):401–409
Von der Gracht H (2012) Consensus measurement in Delphi studies: review and implications for future quality assurance. Technol Forecast Soc 79(8):1525–1536
Iqbal S, Pipon-Young L (2009) The Delphi method. Psychologist 22:598–600
Hansen MP, Bjerrum L, Gharn-Hansen B, Jarbol DE (2010) Quality indicators for diagnosis and treatment of respiratory tract infections in general practice: a modified Delphi study. Scand J Public Health 28:4–11
Lai L, Flower A, Moore M, Lewith G (2015) Developing clinical practice guidelines for Chinese herbal treatment of polycystic ovary syndrome: a mixed-methods modified Delphi study complement. Ther Med 23(3):430–438
Duffield C (1993) The Delphi technique: a comparison of results obtained using two expert panels. Int J Nurs Stud 30:227–237
Nihtyanova SI, Tang EC, Coghlan JG et al (2010) Improved survival in systemic sclerosis is associated with better ascertainment of internal organ disease: a retrospective cohort study. QJM 103:109–115
Denton CP, Hughes M, Gak N et al (2016) BSR and BHPR guideline for the treatment of systemic sclerosis. Rheumatology (Oxford) 55:1906–1910
Knobler R, Moinzadeh P, Hunzelmann N et al (2017) European Dermatology Forum S1-guideline on the diagnosis and treatment of sclerosing diseases of the skin, part 1: localized scleroderma, systemic sclerosis and overlap syndromes. J Eur Acad Dermatol Venereol 31:1401–1424
Hansi N, Thoua N, Carulli M et al (2014) Consensus best practice pathway of the UK scleroderma study group: gastrointestinal manifestations of systemic sclerosis. Clin Exp Rheumatol 32(6 Suppl 86):S-214-21
Bissell LA, Anderson M, Burgess M et al (2017) Consensus best practice pathway of the UK Systemic Sclerosis Study group: management of cardiac disease in systemic sclerosis. Rheumatology (Oxford) 56:912–921
Lynch BM, Stern EP, Ong V et al (2016) UK Scleroderma Study Group (UKSSG) guidelines on the diagnosis and management of scleroderma renal crisis. Clin Exp Rheumatol 34(Suppl 100):106–109
Hughes M, Ong VH, Anderson ME et al (2015) Consensus best practice pathway of the UK Scleroderma Study Group: digital vasculopathy in systemic sclerosis. Rheumatology (Oxford) 54:2015–2024
Foeldvari I, Culpo R, Sperotto F et al (2021) Consensus-based recommendations for the management of juvenile systemic sclerosis. Rheumatology (Oxford) 60:1651–1658
Jaeger VK, Wirz EG, Allanore Y, Rossbach P, Riemekasten G, Hachulla E, Distler O, Airò P, Carreira PE, BalbirGurman A, Tikly M, Vettori S, Damjanov N, Müller-Ladner U, Distler JH, Li M, Walker UA, EUSTAR co-authors (2016) Incidences and risk factors of organ manifestations in the early course of systemic sclerosis: a longitudinal EUSTAR Study. PLoS One 11(10):e0163894. https://doi.org/10.1371/journal.pone.0163894
Khanna D, Lescoat A, Roofeh D et al (2022) Systemic sclerosis-associated interstitial lung disease: how to incorporate two food and drug administration-approved therapies in clinical practice. Arthritis Rheumatol 74:13–27
Fernández-Lázaro D, Iglesias-Lázaro M, Garrosa E, Rodríguez-García S, JervesDonoso D, Gutiérrez-Abejón E, Jorge-Finnigan C (2023) Impact of innovative treatment using biological drugs for the modulation of diffuse cutaneous systemic sclerosis: a systematic review. Medicina 59:247
Acknowledgements
Not applicable
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
Conceptualization and design: Yasser El Miedany, Mohammed Hassan Abu-Zaid, and Waleed Hassan. Acquisition of data: Yasser El Miedany and Mohammed Hassan Abu-Zaid. Formal analysis: Maha El Gaafary. Investigation: Yasser ElMiedany Methodology: all authors. Writing—original draft: Yasser El Miedany, Mohammed Hassan Abu-Zaid, and Samar Tabra. Final approval of the version to be submitted: all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was performed in accordance with the Helsinki Declaration. This was a multistep process that followed the “Clinical, Evidence-based, Guidelines” (CEG) initiative protocol (ethical approval code: 34842/8/21, ethical board Tanta University) aiming at setting up an actionable clinical gold standard for Treat-to-Target management of rheumatic and bone diseases.
Consent for publication
Not applicable.
Competing interests
The authors declare that Mohammed Hassan Abu-Zaid is the associate editor of the Egyptian Rheumatology and Rehabilitation, and Waleed Hassan, Mohammed Mortada, and Yasser El Miedany are from the editorial board of the journal.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
The flow chart for the selection process of the study.
Additional file 2.
Levels of evidence.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El Miedany, Y., El Hadidi, K., El Menyawi, M.M. et al. Egyptian evidence-based consensus on clinical practice recommendations for the management of systemic sclerosis. Egypt Rheumatol Rehabil 51, 9 (2024). https://doi.org/10.1186/s43166-024-00239-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-024-00239-8